

Endometriosis: Symptoms, Causes and Treatment
What is Endometriosis ?
Endometriosis is a condition where tissue similar to the lining of the uterus, called the endometrium, grows outside the uterus. It is a chronic and often painful condition. Endometriosis is a common yet often overlooked condition that can significantly impact a woman’s life. Recognizing the symptoms, seeking timely medical attention, and exploring treatment options are crucial steps in managing this condition effectively.
Within the female reproductive system, we have the uterus, two tubes, and two ovaries. The uterine lining, known as the endometrium, thickens each month in preparation for potential pregnancy under the influence of hormones released by the ovaries. If pregnancy doesn’t occur, the endometrial lining sheds, resulting in menstrual periods. Essentially, menstrual periods consist of this shedding endometrial tissue mixed with blood and mucus. In endometriosis this endometrial tissue exists outside the uterus. It may attach to the surface of the ovaries, the Fallopian tubes, or other abdominal organs. This endometrial tissue outside the uterus behaves similarly to the tissue inside the uterus. It thickens, grows, and sheds each month. However, unlike the uterine lining, which can expel the bleeding through the cervix, the tissue outside, within the abdominal cavity , has no escape route. Consequently, blood accumulates within the abdominal cavity, forming sizable blood-filled cysts referred to as endometriotic cysts or “chocolate cysts” due to their brownish color. This trapped blood induces intense pain and discomfort. Additionally, it irritates the surrounding tissues, causing inflammation. Prolonged exposure to this blood can lead to tissues and organs adhering to one another, forming adhesions.
How Common is Endometriosis ?
Endometriosis affects a significant number of women, but due to the requirement for a surgical procedure (typically laparoscopy) for diagnosis, the exact prevalence is unknown. Roughly 6 to 10% of all women are diagnosed with endometriosis, with higher percentages among women experiencing infertility (25 to 50%) and chronic pelvic pain (75 to 80%). This condition can develop during adolescence, but it is most commonly diagnosed around the age of 27.

Common Locations of Endometrial Tissue Implants
Endometrial tissue, or implants, can be found in various locations within the body, including:
- Ovaries
- Ligaments that support the uterus
- The spaces between the rectum and vagina, cervix, or the space between the bladder and uterus
Less common locations for these implants include the fallopian tubes, the outer surfaces of the intestines, the ureters (tubes connecting kidneys and the bladder), the bladder, and even the vagina. In rare cases, endometrial tissue can develop on the membranes covering the lungs (pleura), the sac around the heart (pericardium), the vulva, cervix, or surgical scars in the abdomen.
These implants, like normal endometrial tissue, respond to hormonal changes in the menstrual cycle. They can bleed and cause pain, especially during and before menstrual periods. The severity of symptoms and their impact on fertility and organ function can vary significantly among individuals.
As endometriosis progresses, the implants may grow gradually and spread to new locations. The quantity of tissue and the pace of progression can vary. Implants may either remain on the surface of structures or penetrate deeply, forming nodules.
Risk Factors for Endometriosis
While any woman can develop endometriosis, certain factors increase the risk of the disease:
- Family history: Women with a mother, sister, or daughter who has endometriosis are at a higher risk.
- Women who gave birth for the first time after age 30.
- White women.
- Women with an abnormal uterus.
Causes of Endometriosis
The exact cause of endometriosis is still uncertain, but several theories exist:
- Retrograde Menstruation: Some theorize that during menstruation, small endometrial tissue pieces may flow backward through the fallopian tubes into the abdominal cavity, rather than exiting the body through the vagina.
- Transport through Blood or Lymph: Another theory suggests that endometrial cells can be transported to different locations through blood or lymphatic vessels.
- Cellular Transformation: It’s also possible that cells outside the uterus may transform into endometrial cells.
- Genetic Factors: Endometriosis tends to run in families, hinting at a genetic component.
Endometriosis can have a hereditary component, being more common among first-degree relatives of affected women. It’s associated with various risk factors, including factors like late first pregnancy, no prior pregnancies, early onset or late cessation of menstruation, short menstrual cycles with heavy and prolonged periods, structural uterine abnormalities, maternal use of diethylstilbestrol (DES) during pregnancy (a drug banned in the United States in 1971).
Conversely, endometriosis appears to occur less frequently in women with characteristics such as multiple pregnancies, later onset of menstruation, extended breastfeeding, prolonged use of low-dose oral contraceptives, and regular exercise, particularly if started before age 15 and involving over 4 hours per week.
Endometriosis Symptoms
- Pelvic pain before and during menstruation: The primary symptom of endometriosis is pelvic pain, typically in the lower abdomen. Pain can fluctuate during the menstrual cycle and tends to worsen just before and during menstruation.
- Other symptoms can include heavy menstrual bleeding, spotting before periods, and, in some cases, irregular menstrual cycles.
- Chronic Pain: Discomfort extending beyond menstruation to affect daily life.
- Painful Intercourse: Pain or discomfort during sexual activity.
- Infertility: Endometriosis can also lead to infertility, with misplaced tissue blocking the passage of eggs from the ovaries to the uterus. Even mild endometriosis may result in infertility, but the exact mechanism remains unclear.
- Fatigue
Misplaced endometrial tissue is sensitive to hormones, like estrogen and progesterone, producing pain, inflammation, and, sometimes, cramps. Pain intensity doesn’t necessarily correlate with the quantity of tissue. Some women with minimal tissue have severe pain, while others with extensive tissue may remain asymptomatic.
Symptoms can also differ based on the implant location. For example:
- Large Intestine: Symptoms may include abdominal bloating, painful bowel movements, diarrhea or constipation, and rectal bleeding during menstruation.
- Bladder: Symptoms may comprise pain above the pubic bone, painful urination, blood in urine, and a frequent urge to urinate.
- Ovaries: Blood-filled masses (endometriomas) may form, which can rupture and cause sudden, severe abdominal pain.
Endometrial tissue bleeding and irritation can result in scar tissue, potentially forming fibrous adhesions between abdominal structures. These adhesions may affect organ functionality and, in rare cases, block the intestines. During pregnancy, endometriosis may become inactive, and after menopause, symptoms tend to decrease due to declining estrogen and progesterone levels.
Endometriosis vs Adenomyosis
Adenomyosis is a condition in which the uterus enlarges because the inner lining, which typically develops inside the uterus, starts growing within the muscular tissue. This displacement can cause intense menstrual pain as blood seeps through the uterine muscular walls and collets there forming small cysts.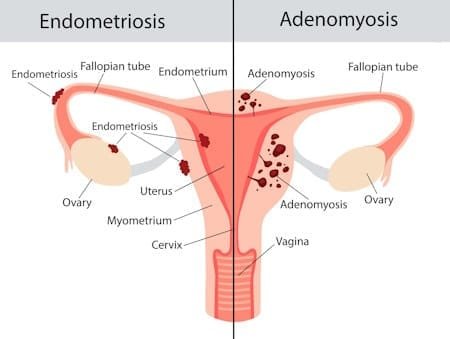
Both Adenomyosis and Endometriosis are conditions related to the uterine lining, which can easily be confused due to their similarities. Both disorders involve abnormalities in the way the uterine lining is shed and often result in excruciating menstrual pain. Because of their close resemblance, patients frequently go undiagnosed or face misdiagnoses for extended periods. Unfortunately, there is a common misconception that painful periods are a normal part of a woman’s experience, leading many to refrain from discussing their symptoms with their healthcare providers.
The key differentiation between adenomyosis and endometriosis lies in where and how the uterine lining is shed. Adenomyosis involves the growth and shedding of the lining within the muscular tissue of the uterus, as opposed to the internal wall. In contrast, endometriosis leads to the growth and shedding of the lining on the exterior of the uterus.
Endometriosis Diagnosis
Diagnosing endometriosis can be challenging due to a lack of awareness among both patients and healthcare providers. However, the following methods can facilitate diagnosis:
- Medical History: A thorough medical history, including a discussion of symptoms, is instrumental.
- Physical Examination: A pelvic ultrasound can provide valuable insights.
- Laparoscopy: A surgical procedure called laparoscopy is considered the gold standard for diagnosing and treating endometriosis. It involves making small incisions and using a thin viewing instrument (laparoscope) to visualize the abdominal cavity. Depending on the location of misplaced endometrial tissue, various diagnostic procedures may be used. This includes a biopsy during a pelvic examination, insertion of a flexible viewing tube through the anus for examining the lower intestine, rectum, and anus (sigmoidoscopy), or the bladder (cystoscopy). In some cases, a larger abdominal incision (laparotomy) may be necessary.
Other tests may include:
- Biopsy. For this test, a small tissue sample is removed from the body during laparoscopy and examined in laboratory.
- Ultrasound: This imaging test employs high-frequency sound waves to generate images of the organs.
- Computed Tomography (CT Scan): A CT scan is an imaging test that utilizes X-rays and computer technology to produce detailed images of the body, revealing information about bones, muscles, fat, and organs. It can identify issues that might not be visible on a standard X-ray.
- Magnetic resonance imaging (MRI). This imaging test provides a two-dimensional view of organs or tissue.
Doctors may suspect endometriosis in women with typical symptoms or unexplained infertility. During pelvic examinations, tenderness or lumps near the uterus may be detected. Ultrasonography or magnetic resonance imaging (MRI) can help evaluate endometriosis noninvasively, mainly to check for endometrial cysts (endometriomas). However, their diagnostic utility is limited.
Laparoscopy remains the primary method for confirming endometriosis diagnosis. It involves examining the abdominal cavity using a laparoscope inserted through a small incision. Sometimes, electrocautery or laser therapy is used to destroy or remove endometrial tissue. The procedure usually causes mild to moderate abdominal discomfort, with patients resuming regular activities within a few days.
Biopsies may be necessary if abnormal tissue is discovered during laparoscopy. A sample is removed and examined under a microscope. Occasionally, a larger abdominal
- Fertility Evaluation: When infertility is a concern, tests are conducted to determine if endometriosis is the cause or if other issues, such as problems with the fallopian tubes, are contributing.
Endometriosis Stages
- Endometriosis Stages: Doctors classify endometriosis into stages based on factors like the quantity, location, and depth of misplaced tissue, as well as the presence of endometriomas and adhesions. Stages range from:-
- Stage 1 minimal
- Stage 2 mild
- Stage 3 moderate
- Stage 4 severe
- Chances of Pregnancy: To estimate the likelihood of pregnancy in women with endometriosis, doctors consider various factors, including the stage of endometriosis, the woman’s age, duration of infertility, prior pregnancies, and the functionality of reproductive organs.
Endometriosis Diet
While the exact cause of endometriosis is still unknown, it’s considered an estrogen-dependent inflammatory disease. Therefore, a diet that’s low in inflammation and estrogen could potentially help manage this condition. Here are some dietary recommendations to help alleviate the symptoms of endometriosis:
- Increase Omega-3 Fats: Omega-3 fats, found in fatty fish, nuts, seeds, and plant oils, have anti-inflammatory properties. These fats can help reduce pain and potentially slow the progression of the disease.
- Limit Red Meat: Red and processed meats are associated with increased inflammation and higher estrogen levels, exacerbating endometriosis symptoms. Reducing red meat consumption may help alleviate discomfort.
- Consume Fruits, Vegetables, and Whole Grains: A diet rich in fruits, veggies, and whole grains provides essential vitamins, minerals, fiber, and antioxidants. High fiber intake can help lower estrogen levels, which can be beneficial for managing endometriosis.
- Restrict Alcohol and Caffeine: While the scientific evidence is not conclusive, many individuals report symptom relief when avoiding alcohol and caffeine.
- Avoid Trans Fats: Trans fats are known to be inflammatory and can exacerbate endometriosis pain and symptoms. These fats are commonly found in processed and fast foods, baked goods, and reheated oils.
- Consider a Gluten-Free Diet: Gluten, a protein found in wheat, barley, and rye, can lead to an increased inflammatory response. Reducing gluten intake may help manage symptoms.
- Try a Low FODMAP Diet: FODMAPs are specific types of carbohydrates found in certain foods that can trigger digestive symptoms. While initially designed for individuals with irritable bowel syndrome (IBS), a low FODMAP diet may also be beneficial for those with endometriosis.
Supplements for Endometriosis
In addition to a healthy diet, certain supplements may help alleviate endometriosis symptoms:
- Vitamin A, C, and E: These vitamins can assist in reducing oxidative stress and inflammation, providing pain relief.
- Zinc: Zinc is known for its anti-inflammatory properties.
- Curcumin (Turmeric): Curcumin, found in the spice turmeric, is a potent anti-inflammatory component that may help reduce estrogen production.
The Importance of Exercise
Regular exercise can help reduce estrogen levels and trigger the release of feel-good hormones. Engaging in activities that make you happy can have a positive impact on your endometriosis symptoms.
Alternative Therapies
Alternative treatments such as relaxation techniques (meditation, yoga), acupuncture, massage, and other forms of stress reduction can be valuable in managing pain and improving overall well-being.
Endometriosis Treatment
1. Medical Approaches to Endometriosis Treatment
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): Typically, NSAIDs are used for pain relief, especially when symptoms are mild and pregnancy is not planned.
- Ovarian Activity Suppression:
- Birth Control Pills: Combining various medications, birth control pills regulate endometrial tissue growth and can lead to lighter periods.
- Progesterone: Progesterone-based treatments, such as oral medications or intrauterine devices (IUDs) like Mirena, can help thin the endometrial tissue.
- GnRH Agonists or Antagonists: These medications block ovarian hormones, inducing a temporary menopausal state that reduces endometrial tissue growth and bleeding.
- Danazol: Danazol is an effective treatment for endometriosis, and has comparable efficacy to other hormonal treatments. However, it comes with a range of androgenic (male-like) side effects, such as weight gain, increased body hair growth, and acne.
Medications are utilized to suppress ovarian activity, slowing the growth of displaced endometrial tissue, reducing bleeding and pain. These drugs may not provide a permanent solution, and recurrence often occurs after discontinuation, unless more radical measures are taken to permanently suppress ovarian function.
2. Surgical Procedures for Endometriosis Treatment
- Laparoscopy: For moderate to severe endometriosis, removing or destroying the misplaced endometrial tissue and endometriomas is often the most effective approach. These surgeries are typically performed through laparoscopy via a small incision near the navel. This intervention is considered when:
- Severe lower abdominal or pelvic pain persists despite drug treatment.
- Significant symptoms result from adhesions in the lower abdomen or pelvis.
- Misplaced endometrial tissue obstructs the fallopian tubes.
- Endometriomas are present.
- Endometriosis leads to infertility, and the patient wishes to conceive.
- Pain occurs during intercourse.
- Endometrial Tissue Removal: During laparoscopy, misplaced endometrial tissue can be removed or destroyed. Techniques such as electrocautery or laser therapy are employed for this purpose. In some instances, abdominal surgery with an incision into the abdomen may be necessary.
- Removal of Endometriomas: Ovarian cysts caused by endometriosis, known as endometriomas, are usually removed because this approach reduces the risk of recurrence compared to draining the cysts.
- Preserving Fertility: During surgery, the aim is to remove as much misplaced endometrial tissue as possible without harming the ovaries, thus preserving the patient’s fertility. Depending on the stage of endometriosis, 40 to 70% of women who undergo this surgery may achieve pregnancy. In cases where complete removal of the tissue is impossible, a GnRH agonist may be administered, but its impact on pregnancy rates is uncertain. Some women with endometriosis can opt for assisted reproductive techniques like in vitro fertilization to increase their chances of conceiving.
- Hysterectomy: For women who don’t plan to become pregnant and experience intractable abdominal or pelvic pain, hysterectomy without removal of the ovaries (salpingo-oophorectomy) may be considered.
- Hysterectomy with Bilateral Salpingo-Oophorectomy: In certain situations, both ovaries and the uterus may need to be removed. This procedure induces menopause due to decreased estrogen levels. For women under 50, estrogen supplementation is often provided to alleviate menopausal symptoms but has to be balanced with the risk of recurrence of symptoms . Progestins may also be prescribed to prevent the growth of any remaining misplaced endometrial tissue. In women over 50, a progestin alone can manage persistent symptoms after ovary removal.
- Definitive Treatment: Hysterectomy with bilateral salpingo-oophorectomy is considered when women near menopause or those who don’t intend to become pregnant desire a definitive treatment for endometriosis. This approach aims to eliminate the disorder permanently, particularly when it has recurred multiple times.
Endometriosis Self-Care
Endometriosis can be a difficult condition to deal with, both physically and emotionally, These simple steps that can help ease the pain of endometriosis:
- Rest, relaxation, and meditation
- Warm baths
- Regular exercise
- Prevent constipation
- Use of heating pad or hot water bottle on your belly
Can Endometriosis cause Cancer?
Endometriosis itself is not dangerous or cancerous. However, it can significantly affect one’s quality of life, leading to severe pain, fatigue, and emotional distress.
Can Pregnancy cure Endometriosis?
While it’s true that conditions such as pregnancy, breastfeeding, and menopause temporarily halt the menstrual cycle, including endometrial tissue growth, this effect is not permanent. Endometriosis often returns after these periods.





")


