
Episiotomy and Vaginal Tears during Childbirth
During childbirth, the vagina stretches to allow the baby to be born. The entrance to the vagina and the skin between the vagina and the anus, called the perineum, are very elastic and stretch to accommodate the baby’s head or any other part of the baby that comes out first. Episiotomy and vaginal tears are potential outcomes of this process. Understanding this can help you prepare for what might happen and how it can be taken care of for your health.
What’s the difference between an episiotomy and a vaginal tear ?
An episiotomy is a surgical cut made by a doctor or midwife through the muscular area between the vagina and the anus, also known as the perineum. It is done to widen the opening and potentially prevent a more severe tear. Episiotomy used to be a standard procedure during childbirth; however, it is no longer routinely performed and is now only carried out in approximately one out of seven deliveries.
A vaginal tear occurs when the baby stretches the vagina during birth to the point where the skin of the perineum strains and tears. Most women experience some degree of vaginal tearing during childbirth.
Types of episiotomy

The two most common types of episiotomy are:
- Midline: A cut made from the vagina directly toward the anus.
- Mediolateral: A cut made from the vagina at an angle off to one side of the anus. This type is more common than the midline.
When might I need an episiotomy?
According to NICE (the National Institute for Health and Clinical Excellence), a routine episiotomy should not be performed during spontaneous vaginal birth. An episiotomy should only be considered necessary for you or your baby if:
- The baby appears to be in fetal distress, meaning there is a significant increase or decrease in the baby’s heart rate, posing a real risk to the baby’s life or well-being if not born quickly.
- There is a clinical need for an assisted birth, such as the use of forceps or a vacuum extractor (ventouse).
- Breech birth, which means the baby is not being born head first.
- You’re having a very long labor and are exhausted.
- You have a large baby.
- You have a serious health condition and need a fast labor and birth to ensure your safety.
How is an episiotomy performed?
An episiotomy is usually a simple procedure. The area around the vagina is numbed with local anesthesia to ensure you don’t feel any pain. If you’ve already had an epidural, the anesthesia can be “topped up” before the cut is made.
Whenever possible, the doctor or midwife will make a small diagonal cut from the back of the vagina, directed downward and outward to one side. After the baby is born, the cut is stitched together using dissolvable stitches.
Types of vaginal tear
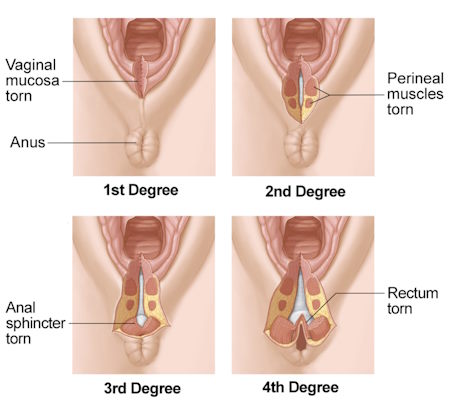
During childbirth, most women (up to 90%) experience some degree of tearing. Most tears occur in the perineum, the area between the vaginal opening and the anus. Tears are classified into degrees based on their size and effect:
- First-degree vaginal tears: These involve the skin of the perineum and the back of the vagina. These tears are often small and don’t require stitches. They heal naturally.
- Second-degree vaginal tears: These involve the skin, back of the vagina, and muscles of the perineum. These tears need to be stitched closed.
For some women, up to nine out of 100 (9%) may experience a more extensive vaginal tear. This can be classified as:
- Third-degree vaginal tears: These involve the skin, back of the vagina, muscles of the perineum, and extend partially or completely through the anal sphincter. Stitches are required to close these tears.
- Fourth-degree vaginal tears: These are similar to third-degree tears but extend into the inner wall of rectum. Stitches are needed to close these tears.
Occasionally, a tear may occur at the top of the vagina, known as a periurethral laceration. These tears are often small and may only require a few stitches, if any.
Is it possible to predict a third or fourth-degree vaginal tear?
It is not possible to predict or prevent these types of vaginal tears completely. However, certain factors may indicate a higher likelihood of experiencing a third- or fourth-degree vaginal tear, such as:
- One of your baby’s shoulders becoming stuck behind your pubic bone.
- The second stage of labor lasting longer than expected (from full dilation of the cervix to birth).
- It being your first vaginal birth.
- Having a large baby (weighing over 8 pounds 13 ounces or 4 kg).
- Induction of labor being required.
- An assisted birth using forceps or a vacuum extractor (ventouse).
What happens after birth?
If a third- or fourth-degree tear is suspected by your obstetrician or midwife or if you had an episiotomy, a detailed examination of your perineum and anus will be conducted. The extent of the tear will be confirmed, and information about surgery and treatment will be provided.
To perform the repair, you will need anesthesia, which can be administered locally, by topping up an existing epidural, or through spinal anesthesia. In some cases, a general anesthetic may be recommended. The damaged anal sphincter and tear will then be stitched together in an operating theater.
Possible incontinence problems
Some women may experience temporary faecal incontinence, which may improve within the first six weeks. If symptoms persist, further investigation or treatment may be required. It is important to discuss any concerns with your GP or during your review appointment with the Consultant.
Healing from a vaginal tear or episiotomy
The healing process for a vaginal tear or episiotomy can take up to a month, with stitches typically dissolving during this time (small tears without stitches may heal faster). During the healing period, mild to moderate pain may persist, and pain relief options should be discussed with your midwife or GP. Painkillers such as paracetamol and ibuprofen (safe for breastfeeding unless specific conditions apply) can be used.
Taking baths in warm water and using a specially designed inflatable cushion can help make sitting more comfortable. If discomfort persists after a few weeks, it is advisable to consult with your midwife, health visitor, or GP.
What can you do to aid your recovery?
To help with the healing process, you can consider the following suggestions:
- Keep the area clean by bathing or showering at least once a day and changing sanitary pads regularly. Wash your hands before and after to reduce the risk of infection.
- After using the toilet, rinse your vaginal area with warm water. Squatting over the toilet rather than sitting on it may reduce the stinging sensation during urination.
- Stay hydrated by drinking at least 2-3 liters of water daily and maintain a healthy balanced diet. This will help prevent constipation and ensure regular bowel movements. If passing stools is particularly painful, a short course of bulk-forming laxatives may be helpful.
- Press a folded sanitary pad against the vagina while straining or having a bowel movement to provide support and reduce pain and pressure on the stitches or tear.
- After passing a stool, wipe from front to back away from the vagina to keep the stitches clean.
- Use ice-packs or ice-cubes wrapped in a towel or cloth on the affected area to relieve pain.
- Perform pelvic floor muscle exercises as soon as possible after birth to increase blood circulation and aid the healing process. Seek physiotherapy advice on specific pelvic floor exercises to do after surgery.
Recovery from a fourth-degree tear
Around 4% of women who deliver vaginally experience a fourth-degree tear, which can cause significant pain and potential anal incontinence. It is important to seek help from your midwife, health visitor, or GP, who can provide assistance and possibly refer you for further medical or surgical advice if necessary. If ongoing problems occur after a tear or episiotomy, a course of antibiotics may be prescribed to reduce the risk of infection.
Long-term effects of a third or fourth-degree vaginal tear
Most women recover well, especially when the tear is recognized and repaired promptly. During the recovery period, some women may experience:
- Perineal pain or soreness.
- Anxiety and concerns about resuming sexual intercourse, even if they did not have a third- or fourth-degree tear.
- Urgency to use the toilet for bowel movements.
- Fear regarding future pregnancies and births.
In rare cases, a fistula (hole) between the anus and vagina may develop after the tear has healed. This can be repaired through additional surgery. Contact your midwife or general practitioner if:
- The stitches become more painful or have an offensive smell (possible signs of infection).
- You experience loss of bowel or wind control.
- You feel an urgent need to rush to the toilet for bowel movements.
- You have any other worries or concerns.
Follow-up appointment
You may be offered a follow-up appointment at the hospital 6-12 weeks after giving birth to ensure proper healing of the stitches. During this appointment, specific questions about urine and bowel functions will be addressed. If any complications arise, you may be referred to a specialist. This appointment provides an opportunity to discuss concerns, including sexual intercourse.
Sex after a vaginal tear or episiotomy
Resuming your sex life after a cut or tear can be a nervous experience. Studies have found that many women who had an episiotomy reported initial pain during intercourse, but this often improved over time. It is important to communicate your concerns with your partner, and if pain during intercourse or at any other time persists despite apparent healing, consult with your GP or health visitor.
Can vaginal birth be possible in the future after a third or forth degree tear?
The possibility of having a vaginal birth in the future depends on various factors. Your obstetrician will discuss these with you during your follow-up appointment or early in your next pregnancy. If symptoms from the third- or fourth-degree tear persist, you may consider a caesarean delivery. However, if the tear has fully healed without any symptoms, a vaginal birth should be possible.
Could anything have been done to prevent a vaginal tear?
In most cases, it is not possible to prevent a third- or fourth-degree vaginal tear because it cannot be anticipated. Research indicates that although an episiotomy creates more space for the baby to be born, it does not prevent these tears from occurring. However, massaging the perineum during the last weeks of pregnancy has been shown to reduce the likelihood of tearing, stitches, or an episiotomy. You can do this alone or with the assistance of your partner. Here’s how:
- Get comfortable by lying against some pillows on the bed with your knees bent so that you or your partner can reach the perineum.
- Massage a vegetable-based oil into the perineal skin.
- Place your fingers around 5cm (2 inches) inside your vagina and press downwards toward the anus, moving to each side in a U-shaped stretching movement. You may feel a tingling or burning sensation. Hold the stretch for 30-60 seconds, then release.








